Seponere fentanyl hva sier ekspertene
“You should never taper off 75mcg fentanyl patches by dropping to 50 mcg and next week to 25. It’s way to much and much too fast. You can cut them so you can talper off every week by about10mcg at a time. You can also have your doctor forescribe the new FDA approved lucemyra which will take care of the withdrawel” var svaret en fentanyl bruker hadde fått av en lege hun hadde kontaktet.
Norsk legemiddelhåndbok har for fentanyl en seponeringsplan
som starter på 62- deretter 50 i 14 dager, så 37 i 14 dager, så 25 i 14 dager, deretter 12 i 14 dager
Tabellen tar utgangspunkt i en dosering på 50 mg/døgn for morfin og oksykodon depottabletter og på 62 μg/time for Fentanyl depotplaster. Vær oppmerksom på at disse dosene ikke er ekvianalgetiske. Ved høyere utgangsdoser kan det være nødvendig å bruke lengre tid, og ved lavere utgangsdoser kan det brukes kortere tid. Tabellen er hentet fra boken Fas Ut 3 (www.fasut.nu) og er gjengitt med velvillig tillatelse fra Claes Lundgren.
https://www.legemiddelhandboka.no/G27.10.2
…………………………………………………………………………………………………………………….
Nettsiden Relis.no langsom reduksjon
En pasient med kronisk pankreatitt skal seponere fentanyl. Vedkommende bruker i dag et depotplaster med fentanyl 100 mikrogram per time. Lege spør om hvordan dette skal nedtrappes/seponeres.
Svar: Det anbefales å trappe ned langsomt og gradvis med 12,5 mikrogram/time av gangen. Pasienten bør være minst 6 dager på hvert steg, helst 12 dager for å minske risikoen for abstinensreaksjoner. Med 12 dagers intervall og 12,5 mikrogram/time av gangen vil nedtrappingen ta totalt 84 dager/12 uker.
Fentanyl depotplaster har en halveringstid på 20-27 timer. Det vil derfor ta 5-6 døgn fra en doseendring før pasienten oppnår likevekt på det nye dosenivået. Ved endring av dose anbefaler preparatomtalen å titrer opp og ned med enten 12,5 mikrogram/time eller 25 mikrogram/time. Seponering skal skje gradvis. Ved for hurtig nedtrapping er det fare for abstinenssymptomer (kvalme, oppkast, diaré, angst og skjelving). Om pasienten får abstinenser bør man gå tilbake til forrige dosenivå før videre nedtrapping (1).
Det svenske oppslagsverket “Fas ut” anbefaler en langsom nedtrapping av fentanyl depotplaster der pasienten holdes 12 dager på hvert nivå før videre nedtrapping. Oppslagsverket anbefaler å nedtrappe i steg på 12,5 mikrogram/time. Ved eventuelle gjennombruddssmerter i forbindelse med nedtrappingen/seponeringen kan det suppleres med et hurtigvirkende opioid i form av morfin eller oksykodon.’
https://relis.no/sporsmal_og_svar/6-9256?source=relisdb
…………………………………………………………………………………………………………………….
Den svenske Kommersiellt obunden läkemedelsinformation riktad till läkare och sjukvårdspersonal
Förslag på utsättning av opioider
Minska dygnsdosen med 10 procent var femte till var sjunde dag tills man nått 30 procent av ursprungsdosen. Fortsätt sedan genom att ta bort 10 procent av kvarvarande dygnsdos varje vecka. För vissa patienter måste nedtrappningen ske månadsvis istället för veckovis.
https://janusinfo.se/behandling/expertradsutlatanden/analgetikaochreumatologiskasjukdomar/analgetikaochreumatologiskasjukdomar/rekommendationerforutsattningavopioider.5.50544c211605519723dac6b5.html
………………………………………………………………………………………………………………….
Den danske sunnhetsstyrelsen skriver dette om fentanyl seponering
Hvordan: Seponering af opioider bør ske ved gradvis udtrapning efter individuel plan.
Efter kortvarig behandling (< 6 uger) kan der fx nedtrappes med 25 % hver 3.-5. dag.
Efter langvarig behandling kan man som tommelfingerregel reducere døgndosis med 10-20 % med 1-2 ugers mellemrum.
https://www.sst.dk/…/182B6C71101C4804904E4460340A22AA
………………………………………………………………………………………………..
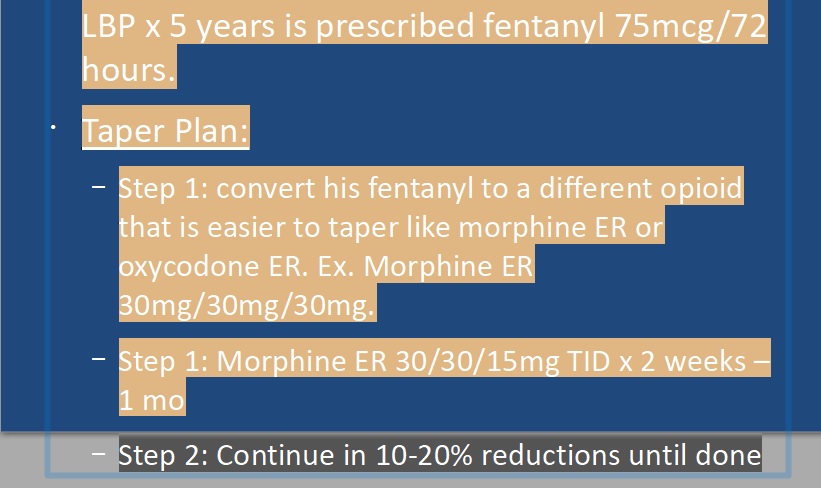
TAPERING LONG-ACTING OPIOIDS
¢ Consider tapering long acting first
¢ Decrease by 10-20% each week
Long acting pill formulations dictate increments of do decrease that are possible
Rate of decrease determined by circumstances of withdrawal: Emergency vs. controlled taper
¢ Allow supply of short acting medications to treat
“breakthrough” symptoms
Build up alternative pain treatment modalities
Comfort medications
¢ Rotate patients on fentanyl to a different long-acting
opioid
https://masspaininitiative.org/files/DGilchrist_MassPI_Spring2017.pdf
……………………………………………………………………………………………………………………….
) If goal is to reduce dose, option to taper further & more gradually may beconsidered at a later point. Tapering plan may be paused/reassessed at any point if pain/function worsens or withdrawal symptoms persist for 1 mos or more. However, the “hold off on further taper & plan to restart taper” conversation should usually have a designated endpoint and be one conversation, not two!
3) Gradual tapers can often be completed in 1-6 months; some may benefit from a longer time frame of 12-24 mons. Literature varies. Some may benefit from opioid agonist therapy.
4) Set a start date! Initial daily dose reductions in the range of 5-10% every 2-4 weeks may be reasonable.1
Once 1/3 of the original dose is reached, smaller dose reductions (e.g. 5% every 4-8 ) may be more optimal for a successful taper.1 (May require formulation change).
https://www.rxfiles.ca/rxfiles/uploads/documents/Opioid-Tapering-Newsletter-Compilation.pdf
………………………………………………………………………………………………………………………………
The Centers for Disease Control and Prevention (CDC) also provides a general opioid medication tapering guideline.
Decrease the original dose 10 percent per week.
Although tapering may be a slow process, it is better than struggling with uncomfortable withdrawal symptoms that may lead to relapse.
If that appears too rapid, going as slowly as 10 percent per month is reasonable.
Make sure the individual has access to psychosocial support, like counseling, during the slow tapering process.
https://riveroakstreatment.com/prescription-drug-abuse/fentanyl/tapering-off/
…………………………………………………………………………………………………………………………
Taper down fentanyl patches by 12-25microgram/hour every 2-4 weeks.
https://www.westsuffolkccg.nhs.uk/wp-content/uploads/2019/01/4.-Fentanyl-Patches-Tapering-Guidance.pdf
……………………………………………………………………………………………………………….
Fentanyl – first rotate to another opioid, such as morphine CR or methadone
https://www.nhms.org/sites/default/files/Pdfs/Safely_Tapering_Opioids.pdf
………………………………………………………………………………………………………………….
https://www.healthtap.com/user_questions/248890-the-duragesic-fentanyl-patch-i-ve-been-on-for-years-is-it-better-to-go-cold-turkey-or-taper
Her kan man stille spørsmål til leger om forskjellige ting.
………………………………………………………………………………………………………………………..Box 1
2017 Canadian Guideline for Opioids for Chronic Non-Cancer Pain: Strategies for opioid tapering2
Gradually reduce 5% to 10% of the morphine-equivalent dose every 2 to 4 weeks with frequent follow-up. Switch the patient from immediate-release to extended-release opioids on a fixed dosing schedule. Collaborate with a pharmacist to assist with scheduling dose reductions.
Alternative methods of tapering include:
Rapid dose reduction in a medically supervised withdrawal centre (may result in severe withdrawal) Switch to methadone or buprenorphine/naloxone and then gradual tapering
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5843113/
……………………………………………………………………………………………………….
7. How quickly should opioids be tapered for patients with CNCP?
The Guideline recommends a rate of 5% to 10% every 2 to 4 weeks. More frequent decreases (e.g., weekly) have been described in other guidelines.3,8 Rapid tapers (immediate or over a few days/weeks) should only be carried out in a medically supervised withdrawal centre, where severe withdrawal symptoms can be managed.2 Patients who have been on opioids for a very long time or are highly anxious may benefit from a much more gradual taper.18 Any decrease in the opioid dose reduces potential harms; the focus should remain on successes to continue to motivate the patient.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5843113/ Litt lengre ned
Individuals coming off fentanyl and other opioids almost always relapse. In one large study in 2010, persons tapering opioids during a nine-month period, whether initially or after a period of substantial improvement, led to nearly universal relapse. This is because tapering by itself doesn’t work and people still experience withdrawal symptoms.
To taper fentanyl effectively, there are a few guidelines that you should follow:
The slower you taper, the fewer withdrawal symptoms you will experience. Use the least amount of medication as possible to feel OK, and avoid taking more. Don’t fear to come off fentanyl (fear affects your brain chemistry negatively).
Make small dose reductions every 10 or 14 days.
The lower you go, the slower you should go.
Always listen to your body and adjust tapering speed as needed.
Your doctor can provide you with fentanyl patches in less and less strength so you can taper properly.
Never cut the fentanyl patches.
Sometimes doctors will switch people on fentanyl patches to a different opioid for the taper process.
https://opiateaddictionsupport.com/how-to-taper-off-fentanyl-patch-without-withdrawal/
…………………………………………………………………………………………………………………….
Å bytte fra fentanyl/Ocycontin/ og tilsvarende med Buprenorfin medikamenter som Norspan kan utløse sterke abstinenser dersom det gjøres for raskt
“If a patient dependent on opioids takes buprenorphine when they have opioid in their system, the buprenorphine will rapidly block the effects of their opioid causing what is termed “precipitated withdrawal.” The severity of this effect varies from mild discomfort to severe distress. This is why there is a washout period for opioid tolerant patients before starting buprenorphine.
Once significant withdrawal has begun the administration of buprenorphine produces relief of withdrawal, anxiolysis, and analgesia. Some patients with significant liver disease (ALT > 5x normal) may not be able to take buprenorphine long-term. Avoid in patients with hypersensitivity to buprenorphine or naloxone.”
Dersom man har brukt store doser med fentanyl/oxycontin eller tilsvarende vil det å bytte til Buprenorfin (Norspan plastre) eller tabletter som inneholder buprenorfin kunne utløse sterke abstinenser. Vanlig praksis er å avslutte behandlingen av fentanyl/oxycontin og så la det gå opp mot 20 timer før man tar i bruk buprenorfin medikamenter. Man må med andre ord først komme i moderat abstinens før man starter opp behandling med buprenorfin. Det er også viktig at man starter med lav dose buprenorfin og så gradvis øker styrken inntil man når tilfredsstillende smertelindring. Å gå direkte fra en full-agonist til en partiell agonist som buprenorfin er, vil kunne gi ekstra tøffe abstinenser og man følger da COWS skjemaet før man setter i gang behandling med buprenorfin medikamenter.
https://www.youtube.com/watch?v=qhsgGWu9HrQ&t=242
https://www.mdcalc.com/cows-score-opiate-withdrawal
While Travis was lucky enough to free himself from withdrawals without returning to opioids, he learned only later that his method of reducing his intake by 25% was far too aggressive. The Centres for Disease Control and Prevention (CDC) actually recommends that opiates be tapered off by 10% per week.
https://www.hotdoc.com.au/practices/blog/tapering-patients-off-pain-medication/
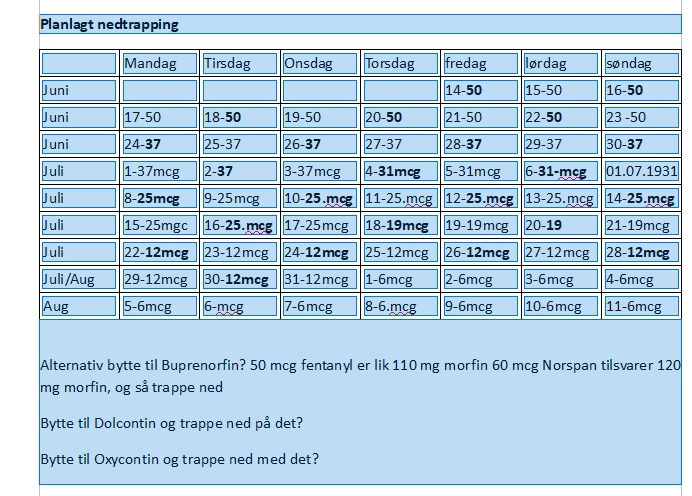
Nedtrappingsplan
How Long Have You Been on the Opiate?
In general, the longer you have been on an opiate, the longer your taper may take. This length is for several reasons, including the likelihood that if you have been on an opiate for a long time, you may be taking a high dose. High doses are common because of opiate tolerance, meaning that over time your body gets used to the low doses, so you need to take higher doses to get the desired effect. As it takes longer to taper off a high dose than a low dose, your taper may take longer if you have been taking the opiate longer. Is the Opiate Short-Acting or Long-Acting?
Short-acting opiates tend to stay in your body for shorter periods than long-acting opiates. Therefore, a taper for a short-acting opiate may be faster than a taper for a long-acting opiate. Understanding the type of opiate is essential to knowing how to taper from it. It has been shown that by using this protocol, withdrawal symptoms can be greatly minimized. If the patient has been on opioids for more than 2 years, however, then you may need to wait as long as a month between tapers, rather than a week, noted Dr. Berna. Chronic pain patients may need to taper slowly so they have time to build in other strategies for living with pain.
![]()